
Eczema concerns?
FREE
Get instant expert guidance with our smart AI platform.
Join Now“Eczema” is a big umbrella. Atopic dermatitis is one type, but so are irritant and allergic contact dermatitis. They can look alike, which is why many people chase moisturizers and steroid creams for months when the real fix is avoiding a hidden allergen or dialing down irritants at work or home. The gold standard for diagnosing allergic contact dermatitis is patch testing, and knowing when to ask for it can save you a lot of trial and error.
This guide gives you quick, practical clues to tell contact dermatitis from atopic eczema, shows common “allergen maps” by body site, explains patch testing (including standard vs expanded panels), and lays out a two-week calm-skin plan you can start today.

Use these patterns as hints—not diagnoses.
Large patch-test networks (e.g., NACDG) consistently report nickel, fragrance mixes, and isothiazolinones among top allergens; MI/MCI drove a well-documented “epidemic” of ACD in the 2010s, with rates falling only after regulatory changes.
What it is: Small amounts of standardized allergens are placed in chambers on your back for 48 hours, then the skin is “read” for delayed reactions at set times. It identifies allergic (not irritant) triggers. Patch testing is the gold standard for ACD.
When to ask for it:
Which panel:
What results look like: You’ll receive a list of positives (for example, “methylisothiazolinone,” “fragrance mix I,” “carba mix”) and synonyms to avoid. That shopping list becomes your long-term prevention plan.
While you arrange care, start this simple plan that helps both contact dermatitis and atopic eczema:
Days 1–3: Strip back
Days 4–7: Friction, fabrics, and laundry
Days 8–14: Product challenge (optional)
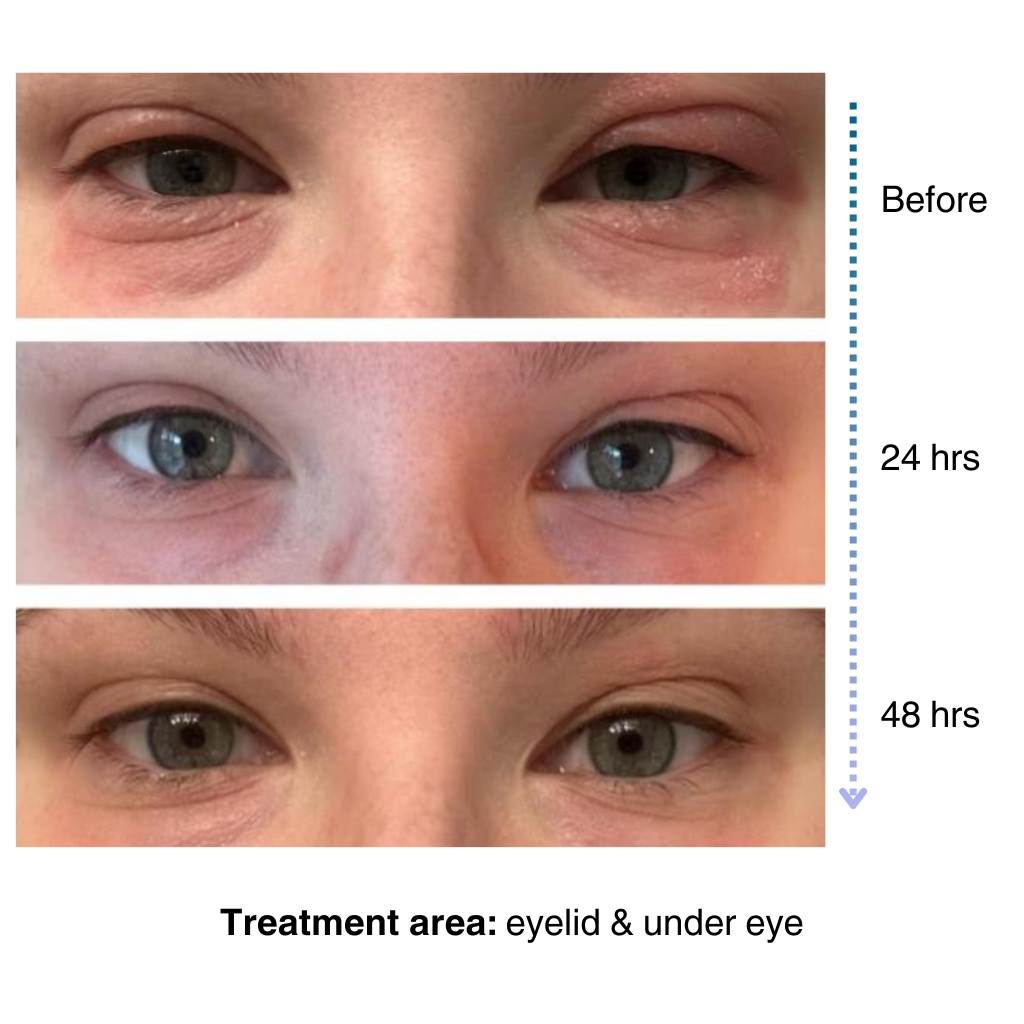
Through the whole two weeks: short lukewarm showers, cleanse only where needed, and moisturize within three minutes after any rinse. If you want a single steroid-free barrier cream that layers well day and night, try NellaCalm Steroid-Free Eczema Cream.
You can absolutely have both, but these patterns point toward irritant contact dermatitis:
ICD is more common than ACD overall, especially on hands and in jobs with “wet work.” Barrier repair plus smarter workflow (sanitize between washes, moisturize after every dry, wear appropriate gloves) is the core fix.
What To Bring To Your Dermatology Visit
If your “eczema” keeps bouncing back in the same spot, or started in adulthood, there is a good chance contact dermatitis is part of the story. Use at-home clues (timing, location, spread) to narrow it, cut fragrance and high-risk preservatives while you calm the skin, and ask your clinician about patch testing ideally with an expanded panel and your own products. Treating inflammation helps today; identifying the allergen (or irritant) prevents tomorrow’s flare.
Can atopic eczema and contact dermatitis coexist?
Yes—and they often do. AD makes the barrier leakier, which can increase the chance of developing contact dermatitis. That is why persistent or odd-pattern rashes in adults with AD warrant patch testing.
Are drugstore “hypoallergenic” labels reliable?
There is no single standard. “Fragrance-free,” short ingredient lists, and specific “free-from” claims guided by your patch-test results are more useful.
Will patch testing flare my skin?
It can cause small, temporary reactions where allergens are placed, which is how clinicians identify positives. Overall it is considered safe and highly informative for ACD.
If I am positive to fragrance mix, can I still use essential oils?
Probably not. Essential oils contain many fragrance components and cross-reactors. Your patch-test report will list synonyms to avoid.
What if my hands are cracked before work every day?
Treat fissures to closure, then protect: sanitize between necessary washes, moisturize after every dry, consider accelerator-free nitrile gloves or cotton liners for long tasks, and rinse/replace damp gloves frequently.
It’s easy to apply and isn’t chalky at all. I’ve been applying it multiple times a day… I’ve tried multiple new products to try and treat my eye eczema, and this is definitely the best I’ve tried so far.
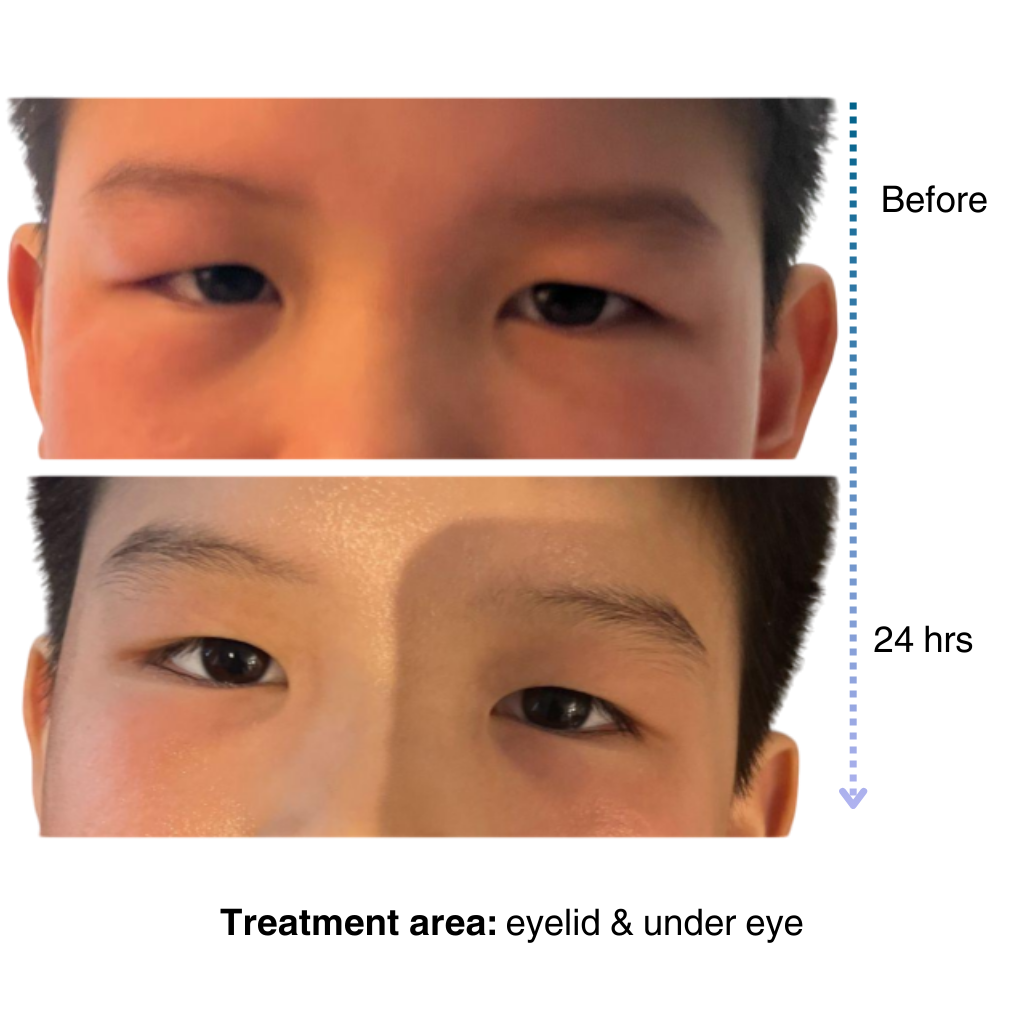
My 7-year old son has been dealing with eczema on his face for a long time, and it’s been so tough to find something that really works…..I’m amazed by the results! Within one day, the redness and rough patches on his face significantly improved…. he doesn’t mind using it at all because it doesn’t sting or feel greasy. – Lily

Get expert advice, exclusive offers, and real stories from people who understand your journey.
Start your skincare journey with an exclusive discount
Practical advice for managing sensitive and eczema-prone skin
Be the first to try our latest technology and product releases
Get 10% off your first order when you sign up
Secure & Private
Instant Access
Premium Content
Like many of you, our eczema journey is personal. That’s why we’re committed to creating a space for the eczema community to share experiences, be empowered through evidence-based solutions, and learn practical tips for daily life.
– Sajjad, Founder & CEO of NellaDerm
