
Eczema concerns?
FREE
Get instant expert guidance with our smart AI platform.
Join NowHormones, heat, sweat, and sleep changes can all push skin off balance. For many, eczema and pregnancy will either calm down or flare—sometimes both in different trimesters. The goal here is a clear, copy-and-paste plan for what you can use, what to avoid, and how to set up nursery and postpartum routines that keep the barrier steady without compromising safety.
Large cohort and review data in Cochrane Library show topical corticosteroids are generally safe in pregnancy; caution mainly applies to high cumulative doses of potent or very potent steroids because of a possible association with lower birth weight. Narrowband UVB phototherapy is widely considered safe in pregnancy and breastfeeding (though long courses can reduce folate, so supplementation is reasonable). For itch control, second-generation antihistamines like cetirizine and loratadine are commonly recommended when needed. Emerging reviews suggest dupilumab has not shown clear pregnancy safety signals, but decisions should be individualized with your dermatology and obstetrics teams.

If you want a single steroid-free base that layers well morning and night, keep a tube of NellaCalm Steroid-Free Eczema Cream at the sink and in your bag.
Usually safe with routine use
Use only with specialist guidance
Avoid
AM
Midday
PM
Laundry can make or break control during eczema and pregnancy. Use fragrance-free liquid detergent, smallest effective dose, and an extra rinse; skip softeners and scent beads that leave residue. Details: Laundry Lessons: How Detergent Decisions Influence Eczema Irritation.
Between night feeds, sweat, and constant handwashing, many notice postpartum flares of face, hands, and flexures.
Breastfeeding compatibility
Hand-care loop for newborn care
Sleep and stress
If rashes localize to a single band, watch strap, eyelids, or hands and do not respond to standard care, allergic contact dermatitis may be layered on top of atopic eczema—very common in new parents using new products. Patch testing (including testing your own products) can end the mystery and simplify your routine.
“My face burns with everything in the first trimester.”
Simplify to one fragrance-free moisturizer. Apply over damp skin. Use mineral sunscreen and press to spread. If still reactive, ask about a short course of a mild steroid or a dermatologist-guided non-steroidal option for the face.
“My hands crack from constant washing.”
Switch to sanitizer between necessary washes, lukewarm water for washes, and moisturize after every dry. Consider cotton liners under nitrile gloves for dish duty.
“Heat makes my itch explode late in pregnancy.”
Time walks for cooler hours, wear breathable layers, and do a quick rinse-and-seal after activity. If widespread, ask about NB-UVB to reduce steroid load.
“I have moderate to severe disease and nothing topical is controlling it.”
Discuss phototherapy first. If still severe, your specialists may review systemic options; early pregnancy data on dupilumab are reassuring but still limited, so shared decision-making is key. JAK inhibitors are off the table.
Days 1–3: Calm and simplify
Days 4–7: Friction and sweat control
Days 8–14: Add light or fine-tune meds
With eczema and pregnancy, your best wins are boring and repeatable: short lukewarm showers, moisturize within three minutes, fragrance-free laundry, and targeted, evidence-based treatments. Low-/mid-potency topical steroids remain first-line; NB-UVB can step in when you need a steroid-sparing option; second-generation antihistamines can help itch with OB approval. Avoid JAK inhibitors, oral retinoids, and other teratogens. Set up the nursery and your sinks for gentle routines now, and you will glide through postpartum with calmer hands and fewer sleepless, itchy nights.
Does pregnancy always worsen eczema?
No. Some improve, others flare. Plan for either and act early.
Can I use my prescription steroid on the belly or breasts?
Yes, with appropriate potency and duration from your clinician. If used on the breast, apply after feeding and wipe before the next feed.
Is dupilumab an option if my disease is severe?
Discuss case-by-case. Current reviews and registries have not shown major safety signals but data remain limited; shared decision-making with dermatology and obstetrics is essential.
What about JAK inhibitors?
Avoid during pregnancy and breastfeeding.
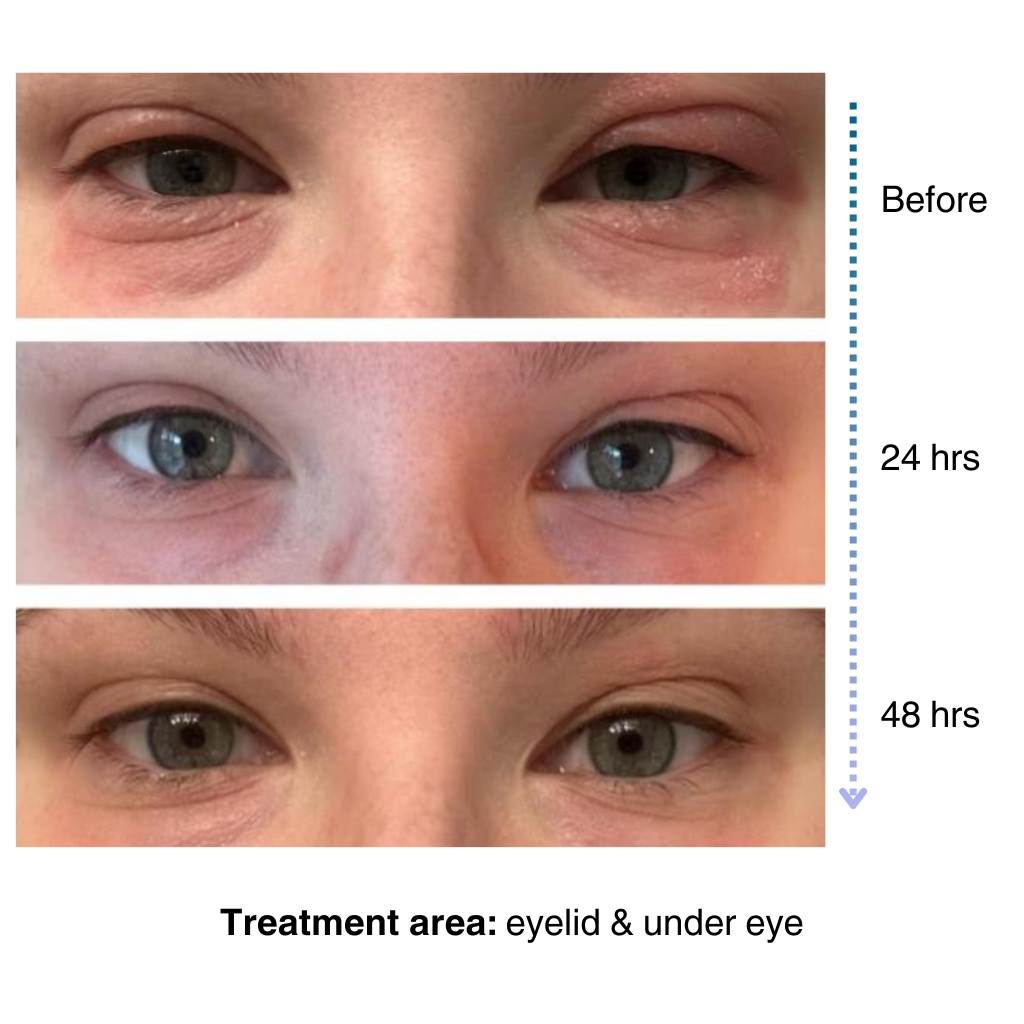
It’s easy to apply and isn’t chalky at all. I’ve been applying it multiple times a day… I’ve tried multiple new products to try and treat my eye eczema, and this is definitely the best I’ve tried so far.
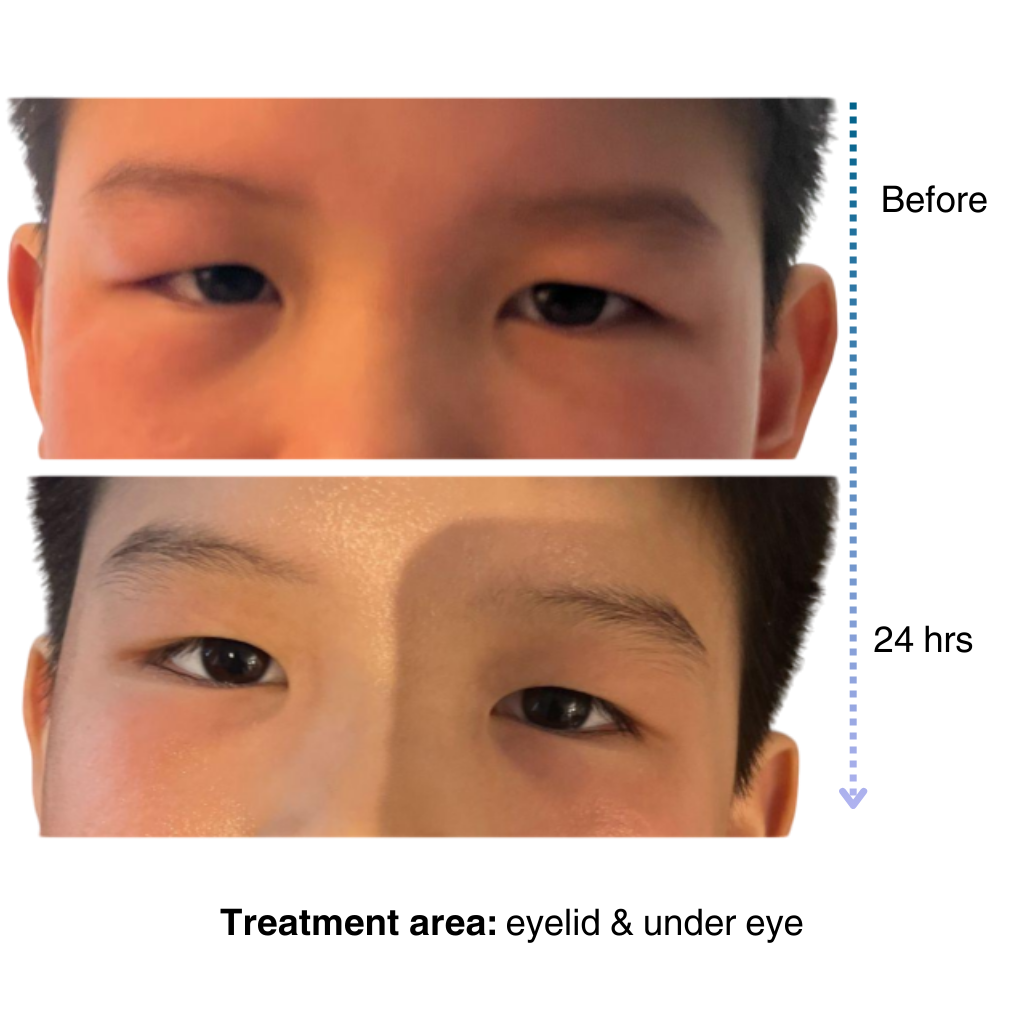
My 7-year old son has been dealing with eczema on his face for a long time, and it’s been so tough to find something that really works…..I’m amazed by the results! Within one day, the redness and rough patches on his face significantly improved…. he doesn’t mind using it at all because it doesn’t sting or feel greasy. – Lily

Get expert advice, exclusive offers, and real stories from people who understand your journey.
Start your skincare journey with an exclusive discount
Practical advice for managing sensitive and eczema-prone skin
Be the first to try our latest technology and product releases
Get 10% off your first order when you sign up
Secure & Private
Instant Access
Premium Content
Like many of you, our eczema journey is personal. That’s why we’re committed to creating a space for the eczema community to share experiences, be empowered through evidence-based solutions, and learn practical tips for daily life.
– Sajjad, Founder & CEO of NellaDerm
