
Eczema concerns?
FREE
Get instant expert guidance with our smart AI platform.
Join NowLED devices are everywhere now, from desk-sized panels to flexible masks. Some people report calmer, less itchy skin after short sessions, so it is fair to ask whether red light therapy for eczema is a smart add-on. The short answer: medical phototherapy remains the gold standard when creams are not enough, and most of that evidence is for narrowband UVB delivered in dermatology clinics. Consumer red or near-infrared LEDs have promising biology but far fewer eczema-specific trials. This guide sets expectations, shows the strongest data we have, and gives a safe, step-by-step plan if you want to run a careful home test.

Recent guidelines and reviews back NB-UVB and other medical phototherapy options for atopic dermatitis, especially when topical care is not enough. Trials and decades of clinical experience support NB-UVB’s effectiveness and safety when supervised. Large ongoing studies continue to refine cost-effectiveness and protocols.
A recent prospective, controlled study using UV-free blue light (≈453 nm) reported significant improvements in EASI and SCORAD after ten full-body sessions, with good tolerability. That does not prove red light will behave the same, but it shows visible light can help some people with AD when delivered at the right dose.
Dermatology reviews describe anti-inflammatory and pro-healing effects from red/near-IR photobiomodulation in several skin conditions, mediated by mitochondrial and cytokine pathways. These mechanisms are relevant to eczema biology, yet high-quality AD-specific trials with red/near-IR LEDs are still sparse. In practice, red light therapy for eczema is best considered a conservative add-on for calm skin, not the main treatment during flares.
For a deeper comparison of medical UV options (different from red LEDs), see our explainer on eczema phototherapy and how clinic vs at-home UV devices are prescribed and monitored.
For more tips and trick on eczema treatments, read our blog post: Eczema Cure Myths vs. Science: What Actually Heals Atopic Dermatitis Long-Term.
Use on calm skin as an adjunct. Stop if you feel heat, prickling, or see new redness that lasts into the next day.
Session template, every other day
Days 1–3
Days 4–7
Days 8–14
Morning
Evening
After exercise or heat
Clinic-based NB-UVB remains the standard when you need a steroid-sparing option with an established track record for AD.
Skin looks pink right after sessions
A brief flush that fades within an hour can be normal. Persistent redness into the next day means the dose or distance is too aggressive. Shorten time or increase distance.
Sting or “pins and needles” during sessions
Stop, cool the skin with a fan, and resume another day at a lower dose. Sessions should never feel hot.
No benefit after two weeks
It may not be your tool. Consider retiring the device and discussing NB-UVB or other guideline-supported options with your dermatologist.
Red light therapy for eczema is a reasonable curiosity in 2026, but it should not displace the basics that actually move the needle: moisturize within three minutes after rinsing, control heat and sweat, treat active inflammation with prescribed topicals, and escalate to NB-UVB or other clinician-guided therapies when needed. If you want to test a home LED panel, keep sessions short, cool, and consistent for two weeks, protect your eyes, and track real outcomes like itch and sleep. If your skin does not vote “yes,” pivot to options with stronger evidence—and keep your barrier routine rock solid.
Is red light therapy for eczema proven?
Not at guideline level. Current recommendations support NB-UVB for AD; consumer red LEDs have intriguing mechanisms but limited eczema-specific trials.
What about blue light devices?
There are small but positive AD studies using UV-free blue light around 453 nm with improved scores after short courses. Devices and doses differ, so results are not guaranteed, but the signal is encouraging.
Can I use red light on my face and eyelids?
Avoid direct eyelid exposure and always wear protective goggles. Keep sessions short and non-heating.
Can I combine red light with my steroid or calcineurin inhibitor?
Yes, but not at the same time on the same spot unless your clinician instructs otherwise. Separate them by day or by hours.
How long until I know if it helps?
If you see no change in itch, sleep, or plaque feel after two weeks of consistent, well-tolerated use, it is reasonable to stop.
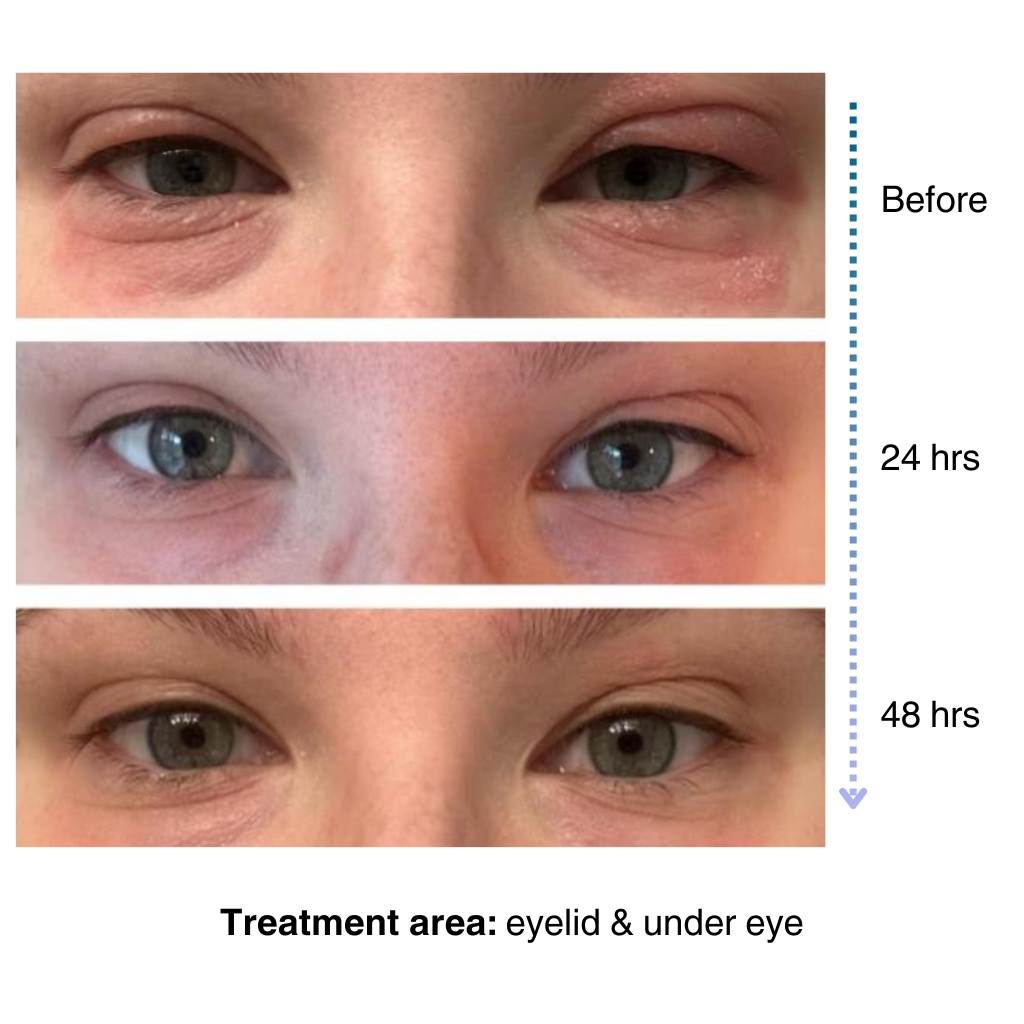
It’s easy to apply and isn’t chalky at all. I’ve been applying it multiple times a day… I’ve tried multiple new products to try and treat my eye eczema, and this is definitely the best I’ve tried so far.
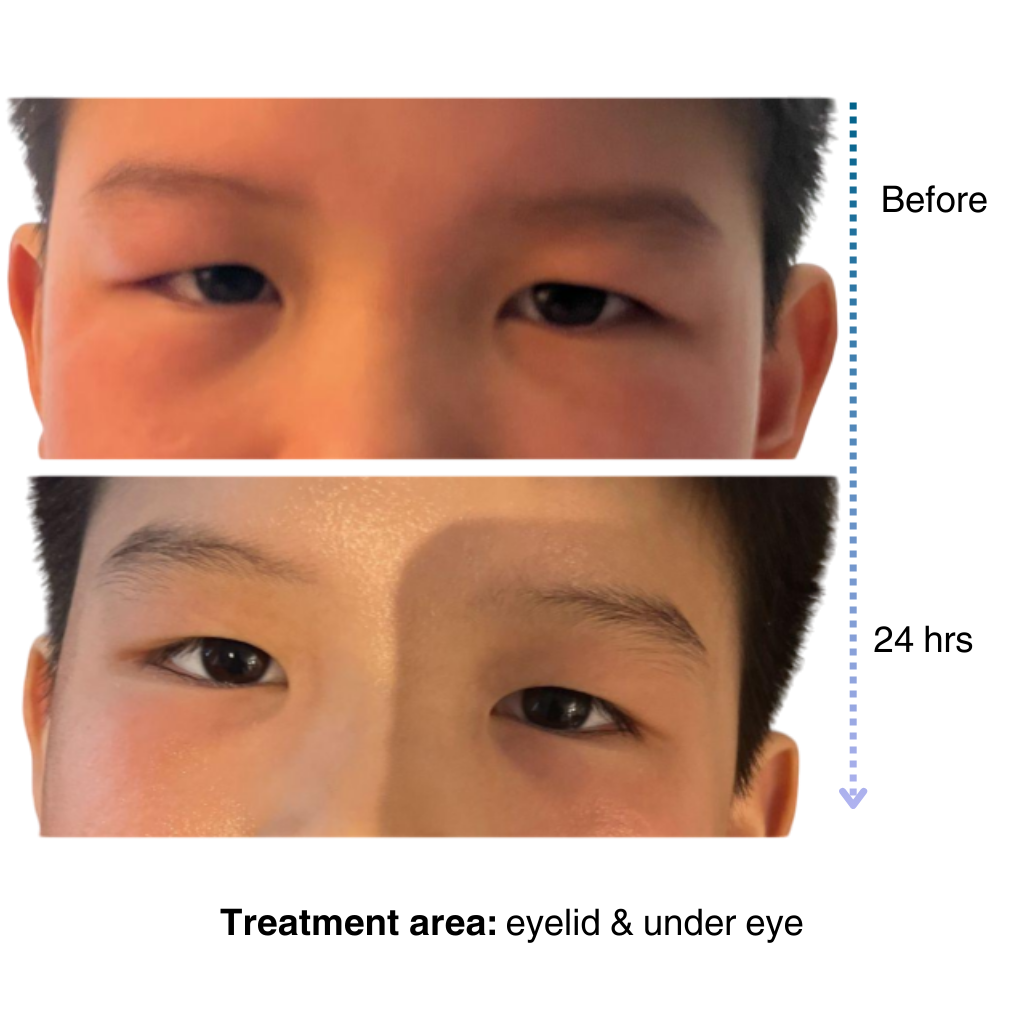
My 7-year old son has been dealing with eczema on his face for a long time, and it’s been so tough to find something that really works…..I’m amazed by the results! Within one day, the redness and rough patches on his face significantly improved…. he doesn’t mind using it at all because it doesn’t sting or feel greasy. – Lily

Get expert advice, exclusive offers, and real stories from people who understand your journey.
Start your skincare journey with an exclusive discount
Practical advice for managing sensitive and eczema-prone skin
Be the first to try our latest technology and product releases
Get 10% off your first order when you sign up
Secure & Private
Instant Access
Premium Content
Like many of you, our eczema journey is personal. That’s why we’re committed to creating a space for the eczema community to share experiences, be empowered through evidence-based solutions, and learn practical tips for daily life.
– Sajjad, Founder & CEO of NellaDerm
