
Eczema concerns?
FREE
Get instant expert guidance with our smart AI platform.
Join NowWhen flares outpace moisturizers and topical prescriptions, eczema phototherapy can be a skin-calming, steroid-sparing option. Dermatologists have used medical UV light for decades to reduce inflammation, itch, and thickened plaques. Today, you can receive UV treatments in a clinic or (with a prescription and supervision) at home using certified devices. This guide explains both routes so you can choose what fits your life, budget, and skin.
A quick note on the basics: phototherapy is not a tanning bed. It uses medical-grade lamps at specific wavelengths, built-in eye and skin protections, and physician-directed dosing schedules.

A 2024 peer-reviewed study from Cureus concludes that NB-UVB and UVA1 are effective and generally safe options for atopic dermatitis, with home phototherapy reasonable only under physician supervision.
Set-up: You’ll stand briefly in a full-body cabinet (or place a hand/foot in a smaller unit). Staff set the dose based on your skin type or your minimal erythema dose test. Eyes are covered with UV-rated goggles; sensitive zones can be shielded with clothing or zinc paste.
Schedule: Usually 2–3 sessions weekly. Many people notice less itch by week 2–4; visible clearing accumulates by weeks 6–12.
Advantages
Limitations
Eligibility: Requires a dermatologist’s prescription and plan. Home therapy is most useful when you responded well in clinic but need maintenance or when access to a phototherapy center is limited.
Devices: From handheld spot devices to small-panel or booth-style NB-UVB units certified for home medical use. Your care team should specify the device, dose schedule, eye protection, and when to pause.
Daily Reality
Advantages
Limitations
Question | Favors In-Clinic | Favors At-Home |
Do you need precise full-body dosing with nurse oversight? | ✓ | |
Is your schedule unpredictable or clinic access difficult? | ✓ | |
Are you early in your treatment journey? | ✓ (to learn response/safety) | |
Are you maintaining results after a successful course? | ✓ | |
Do you have complex health history or prior skin cancer? | ✓ | |
Are your plaques localized (hands, feet, ankles)? | ✓ (targeted devices) | ✓ (handheld units) |
Everyone’s dose curve is different. Missed sessions, intercurrent sun, and flares from heat or stress affect timing—stay in touch with your clinic so they can adjust.
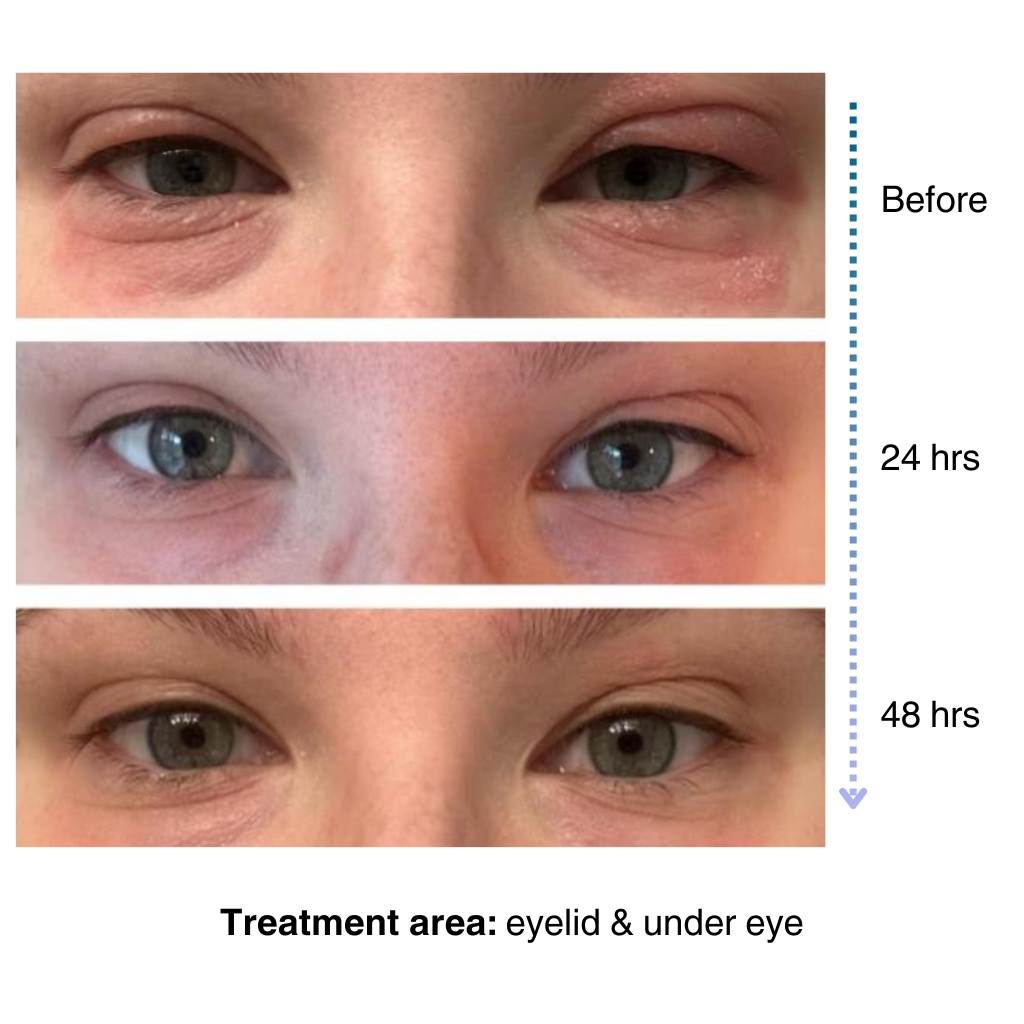
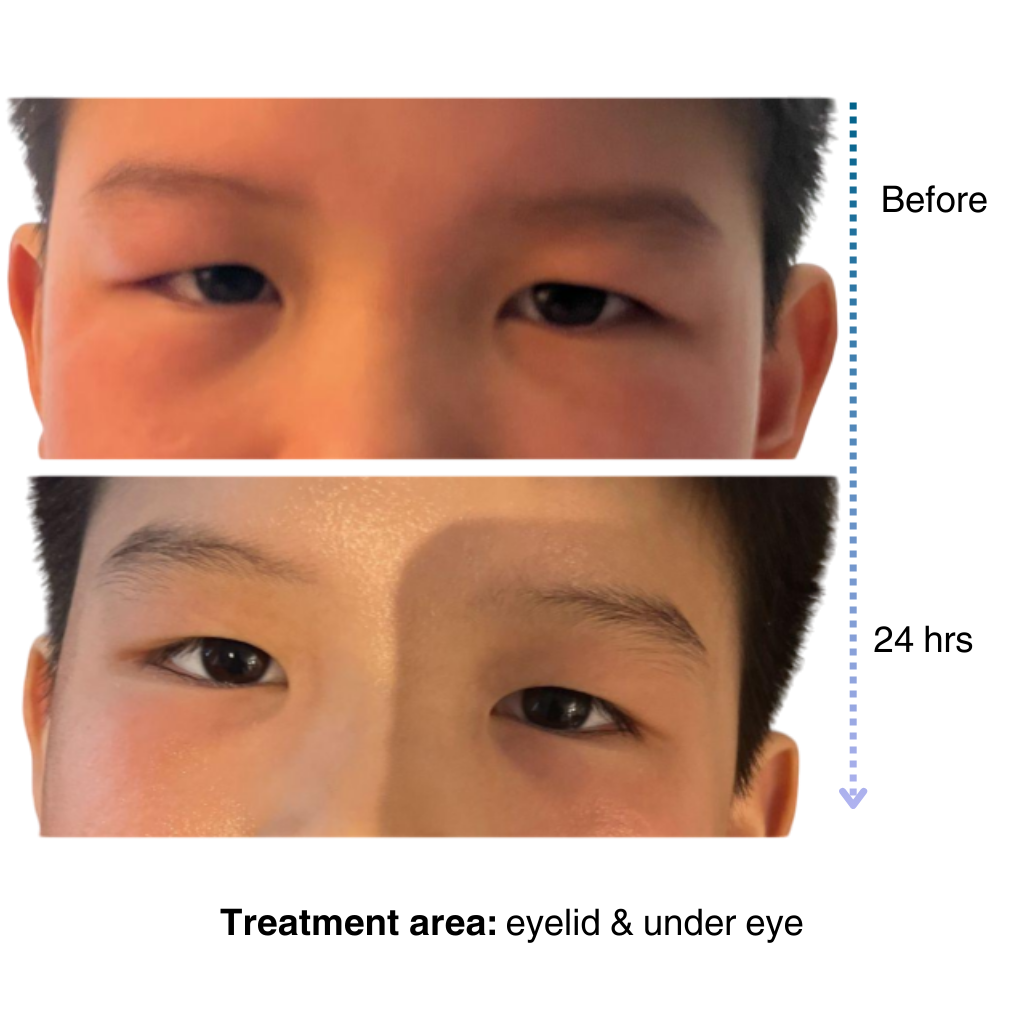
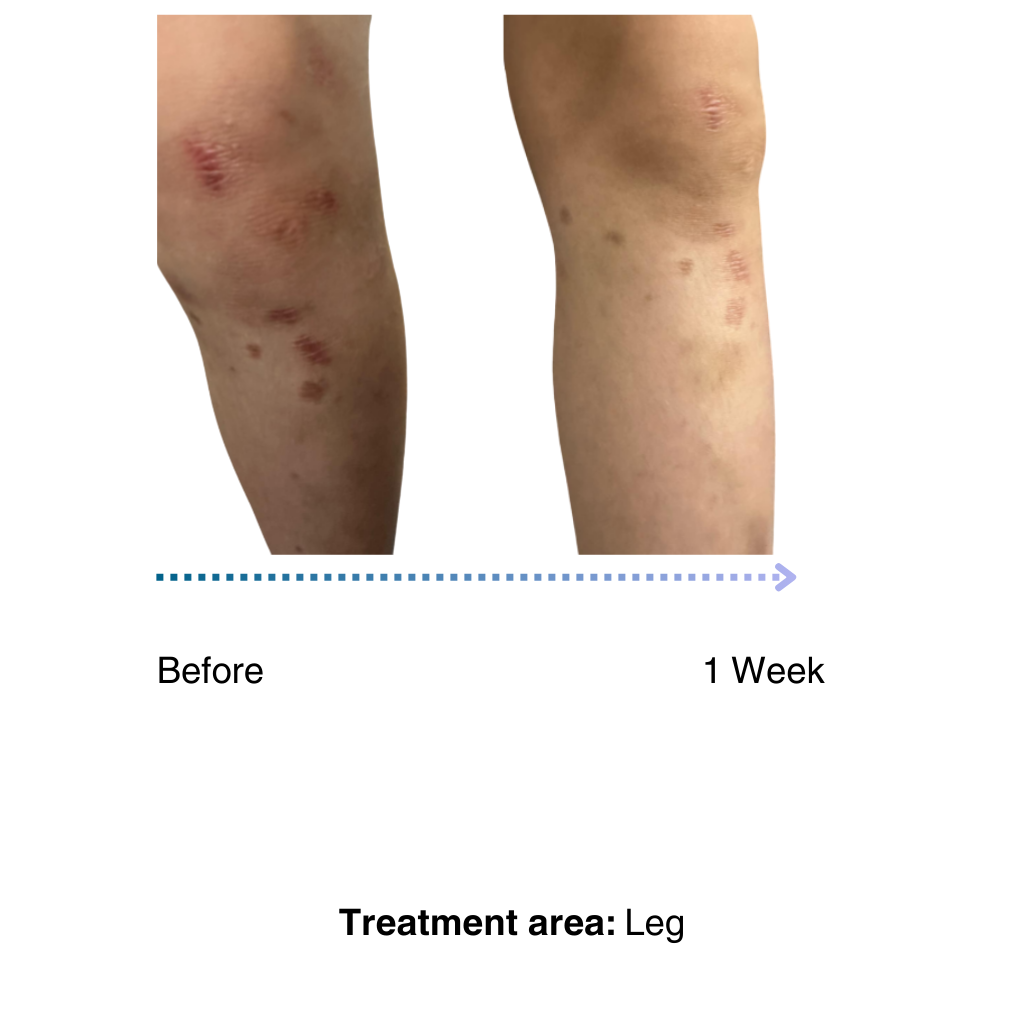
Before
After
For step-by-step daily care that pairs well with phototherapy, see: Skin Minimalism: Simplify Your Eczema Routine
Eczema phototherapy is a proven, non-systemic option that can quiet itch and inflammation when daily care is not enough. Start in a clinic to establish your response and safety, then consider a supervised home unit for convenience and maintenance if it fits your plan. Pair light therapy with consistent moisturizing, smart clothing and laundry choices, and cool, clean bedroom air, and your skin gets the best chance to stay calm.
How is this different from a tanning bed?
Medical devices emit controlled wavelengths and doses with physician oversight; tanning beds are not medical treatments and carry unnecessary risks.
Can children do phototherapy?
Yes, in many centers, using child-specific protocols and protections. Your pediatric dermatologist will guide dosing and frequency.
Will I still need moisturizers or topicals?
Usually, yes. Phototherapy works best on top of a steady emollient routine and may allow you to use fewer steroids or rescue meds over time.
I cannot make it to clinic three times a week. Do I bother?
Talk with your dermatologist about a home NB-UVB plan if you are a good candidate and can follow dosing precisely.
How long do results last
Many people enjoy months of calmer skin after a course; some schedule brief maintenance to stretch results, especially through winter or allergy seasons.
It’s easy to apply and isn’t chalky at all. I’ve been applying it multiple times a day… I’ve tried multiple new products to try and treat my eye eczema, and this is definitely the best I’ve tried so far.
My 7-year old son has been dealing with eczema on his face for a long time, and it’s been so tough to find something that really works…..I’m amazed by the results! Within one day, the redness and rough patches on his face significantly improved…. he doesn’t mind using it at all because it doesn’t sting or feel greasy. – Lily

Like many of you, our eczema journey is personal. That’s why we’re committed to creating a space for the eczema community to share experiences, be empowered through evidence-based solutions, and learn practical tips for daily life.
– Sajjad, Founder & CEO of NellaDerm
