
Eczema concerns?
FREE
Get instant expert guidance with our smart AI platform.
Join Now“Is that eczema or psoriasis?” If you’ve asked this in front of a mirror (or a hurried GP), you’re not alone. Both conditions produce red, scaly rashes, yet mistaking one for the other can cost months of ineffective treatment. This deep dive into eczema vs psoriasis unpacks visual cues, immune pathways, diagnostic tools, and therapy options so you can advocate for accurate care. We’ll also explore overlap syndromes, ethnic-skin nuances, and when to insist on a dermatologist referral. Whether you’re navigating U.S. insurance, Canada’s single-payer system, or the U.K.’s NHS, clear knowledge is your fast-track to relief.

Feature | Eczema (Atopic Dermatitis) | Psoriasis |
Typical onset | Infancy–childhood | Teens–50s |
Immune bias | Th2 / IL-4 & IL-13 | Th1/Th17 / IL-23 & IL-17 |
Hallmark symptom | Relentless itch | Thick, silvery plaques |
Common sites | Elbow flexures, neck, eyelids | Elbows, knees, scalp |
Scale type | Serous, yellowish crust | Dry, micaceous scale |
Family history | Asthma, allergic rhinitis | Psoriasis, psoriatic arthritis |
Meta-omics research found on PMC confirms these immune signatures, guiding targeted therapies.
Eczema arises from a defective barrier (often filaggrin mutations) plus Th2 cytokines. IL-4 and IL-13 weaken tight junctions, letting allergens penetrate. Blocking these signals with dupilumab restores the barrier.
Psoriasis features hyper-proliferative keratinocytes driven by the IL-23/IL-17 axis. IL-17A speeds skin-cell turnover from 28 days to as little as four, creating stacked plaques. That’s why IL-17 or IL-23 biologics (secukinumab, guselkumab) outperform steroids for psoriasis (Frontiers, 2025).
Understanding the eczema vs psoriasis cytokine gulf prevents costly trial-and-error.
Up to 48 % of chronic hand cases are mis-typed (PubMed, 2025). A German group recently trialed a four-gene mRNA classifier that distinguished eczema from psoriasis with 92 % accuracy—promising news for manual-laborers whose livelihoods depend on clear palms.
Paradoxically, some eczema patients treated with cyclosporine develop palmoplantar psoriasiform lesions months later. Recognizing this switch is vital; adding an IL-17 blocker often rescues the case.
In darker Fitzpatrick types, erythema appears violaceous or hyper-pigmented, making scale color more diagnostic than redness.
Coin-shaped plaques on calves can be either nummular eczema or guttate psoriasis. Dermoscopy (next section) helps clarify.
Tool | What it shows | Best-use scenario |
Dermoscopy | Yellow serous crust (eczema) vs white, diffusely distributed scale + dotted vessels (psoriasis) (PMC, 2023). | Palms, soles |
Tape-strip cytokine panel | IL-4/IL-13 vs IL-17 ratios | Research settings |
IL-17A mRNA staining | Positive in palmoplantar psoriasis, negative in eczema | Biopsy-proven uncertainty |
Reflectance confocal microscopy | Parakeratosis patterning | Facial lesions where biopsy leaves scar |
Early adoption of these tools short-circuits the eczema vs psoriasis guessing game.
Category | Eczema mainstays | Psoriasis mainstays |
Barrier care | Daily emollients like NellaCalm Cream | Helpful but adjunct |
Topicals | Calcineurin inhibitors, mild steroids | Vitamin D analogues, high-potency steroids |
Systemics | Dupilumab, JAK inhibitors (abrocitinib) | IL-17, IL-23, TNF-α blockers |
Phototherapy | NB-UVB for widespread itch | NB-UVB or excimer for plaques |
Lifestyle | Allergen avoidance, dust control (see “Eczema During Allergy Season”) | Weight loss (each BMI point lost cuts psoriasis severity 2 %) |
Remember: topical steroids help both for acute flares, but long-term reliance risks skin thinning (eczema) or tachyphylaxis (psoriasis).
Dermatologists can order patch tests, biopsies, and, in Canada/UK, expedite phototherapy referrals.
Yes, you can have both conditions simultaneously. Meta-analysis from Frontiers estimates 7 % coexistence. Managing overlap means blending regimens: emollient-heavy care to protect the barrier (eczema strategy) plus targeted biologics to curb the IL-17 storm (psoriasis strategy). Patient-led tracking apps that log flare triggers, joint pain, and treatment side-effects help your clinician rebalance therapy faster.
Visual clues start the puzzle, but cytokine signatures finish it. Mastering eczema vs psoriasis means marrying barrier repair with immune precision. Use emollients like NellaCalm daily, demand modern diagnostics if rashes defy labels, and remember that correct identification unlocks faster, safer relief.
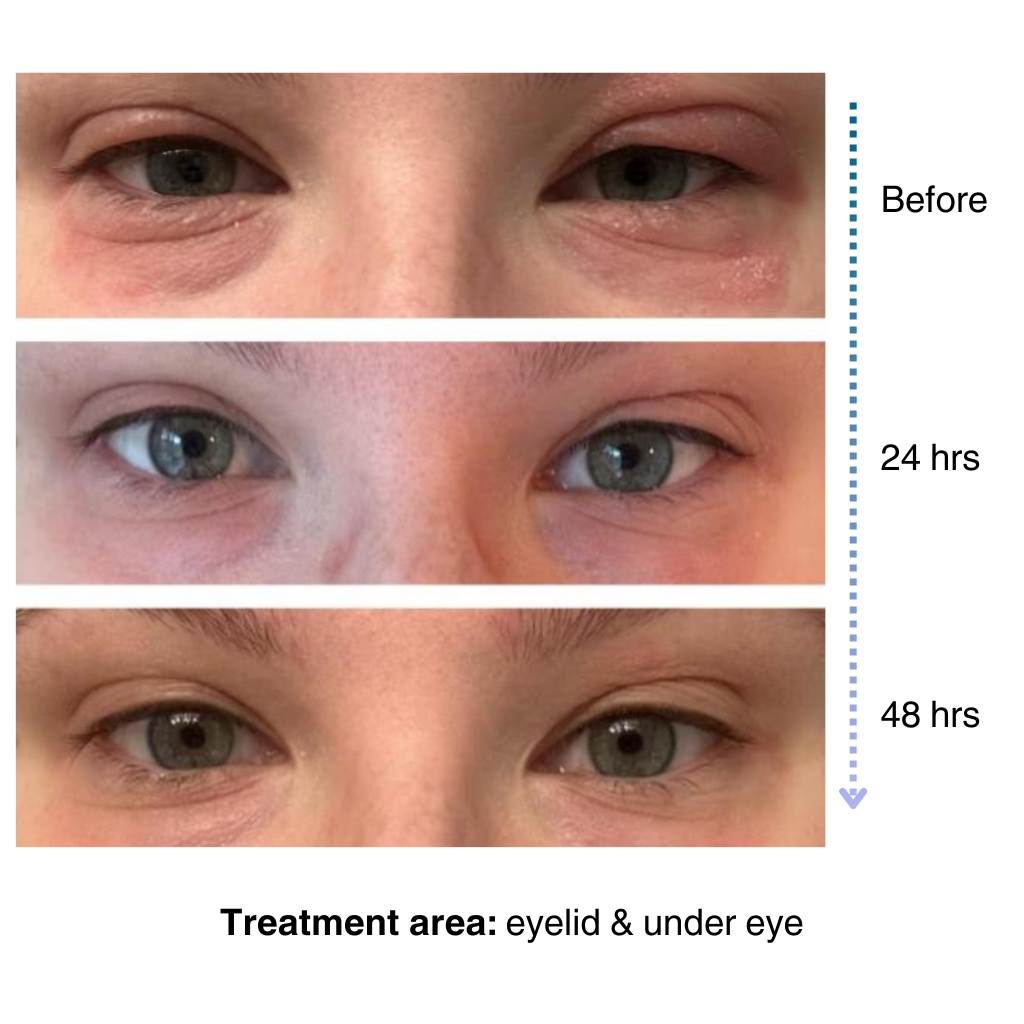
It’s easy to apply and isn’t chalky at all. I’ve been applying it multiple times a day… I’ve tried multiple new products to try and treat my eye eczema, and this is definitely the best I’ve tried so far.
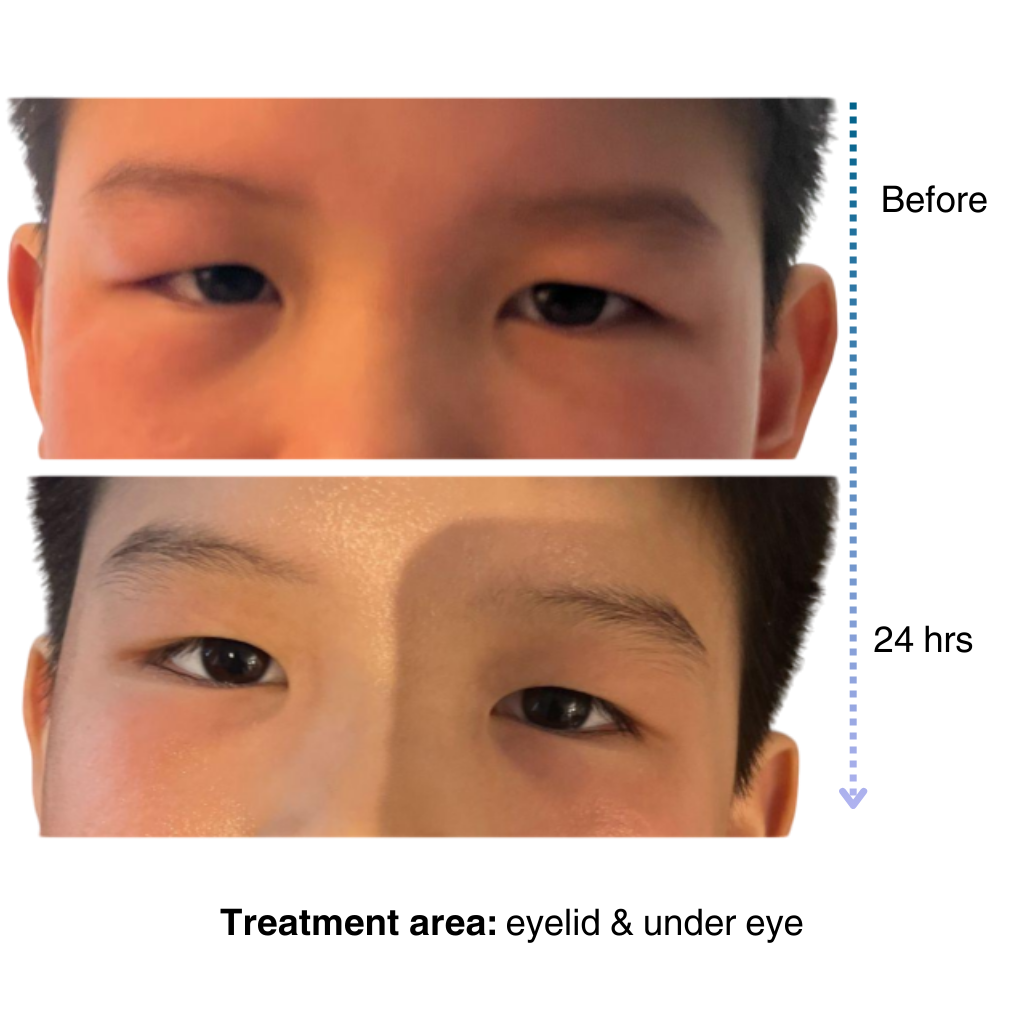
My 7-year old son has been dealing with eczema on his face for a long time, and it’s been so tough to find something that really works…..I’m amazed by the results! Within one day, the redness and rough patches on his face significantly improved…. he doesn’t mind using it at all because it doesn’t sting or feel greasy. – Lily

Like many of you, our eczema journey is personal. That’s why we’re committed to creating a space for the eczema community to share experiences, be empowered through evidence-based solutions, and learn practical tips for daily life.
– Sajjad, Founder & CEO of NellaDerm
