
Eczema concerns?
FREE
Get instant expert guidance with our smart AI platform.
Join NowIf your eczema follows its own calendar: itchy the week before your period, different during pregnancy, or drier and more reactive around menopause, you’re not imagining it. Dermatology research consistently notes that hormonal eczema patterns are common: symptoms often worsen premenstrually, many people flare or newly develop eczema during pregnancy (the “atopic eruption of pregnancy”), and menopausal hormone changes can magnify dryness and itch. Mechanistically, fluctuations in estrogen and progesterone influence immune signaling (notably Type-2 pathways like IL-4 and IL-13) and the skin barrier: two pillars of atopic dermatitis (AD). Understanding those shifts lets you anticipate flares and adjust your routine proactively.
This guide breaks down what’s happening across three milestones, including periods, pregnancy, and menopause, and maps practical steps for hormonal eczema that align with a steroid-sparing, science-backed approach.
In the late luteal phase, which is the week before menstruation, estrogen and progesterone fall. Observational studies and recent reviews link this hormonal drop to increased itch and eczema activity in many patients. Theories include reduced ceramide synthesis (higher transepidermal water loss) and amplified Type-2 inflammation: both of which aggravate hormonal eczema. Clinical data across decades (from classic cohorts to 2025 updates) support the pattern of premenstrual deterioration.
Tip: Some people notice flares with progesterone-only contraception; log symptoms after contraceptive changes and discuss alternatives with your clinician if hormonal eczema worsens. Please review Verywell Health’s article on contraceptive-linked fluctuations for more details.
Pregnancy tilts immune responses and shifts barrier biology. Reviews report that a substantial share of patients flare during pregnancy, and many experience new-onset AD termed atopic eruption of pregnancy (AEP), which includes intense itching in the first two trimesters, often in people with a personal or family history of atopy. AEP is usually benign for parent and fetus but disruptive for quality of life, so symptom-control matters. Refer to ScienceDirect’s article for information on pregnancy-specific dermatoses.
Related reads for expecting parents:
Postpartum: The Fourth Trimester
Hormones swing again; sleep gets scarce; hand-washing spikes. All three can agitate hormonal eczema. Focus on trigger-control you can actually stick to: an emollient at every sink, cotton gloves for overnight hand fissures, and quick “rinse-and-seal” after sweaty feeds or walks. If breastfeeding, confirm medication choices with your clinician; bland emollients are generally compatible, but wipe residual product from the nipple/areola before feeds and reapply after. (Dermatology safety reviews discuss decision-making in lactation.)
Menopause is associated with skin xerosis (dryness) and pruritus, and reviews describe links between the menopausal transition and common dermatoses. Lower estrogen can reduce lipids and water-binding capacity in the stratum corneum, making skin more reactive. While data on whether eczema universally worsens are mixed, many patients report increased dryness and itch that can tip sensitive skin into flares. Targeted barrier care goes a long way for hormonal eczema in midlife.
AD is largely driven by Type-2 inflammation: IL-4 and IL-13 are central, with IL-31 and epithelial alarmins contributing to itch and barrier dysfunction. That’s why IL-4/IL-13-blocking biologics (and JAK inhibitors) can be transformative for moderate-to-severe disease—even when hormonal eczema amplifies symptoms. If topical care and phototherapy aren’t enough, ask your dermatologist about modern options and how they fit with your life stage (family planning, lactation, or menopause).
Build Your Personal “Hormone Map”
Track symptoms against your menstrual cycle (or menopausal timeline), sleep, stress, and weather. Many people find pre-period spikes predictable enough to pre-load care: richer moisturizer, cooler bedroom, and a fragrance-free laundry routine. If pregnancy or menopause changes your pattern, adjust monthly. For a reliable daily baseline, use the step-by-step Eczema-Friendly Skincare Routine.
Hormonal eczema reflects real, biologically plausible shifts in barrier function and immune tone. Pre-period flares often respond to a “buffer week” routine; pregnancy requires safe, steroid-sparing strategies (with NB-UVB as an option); and menopause rewards richer, fragrance-free barrier care. If symptoms remain intrusive, ask about targeted therapies that address the Type-2 drivers of disease.
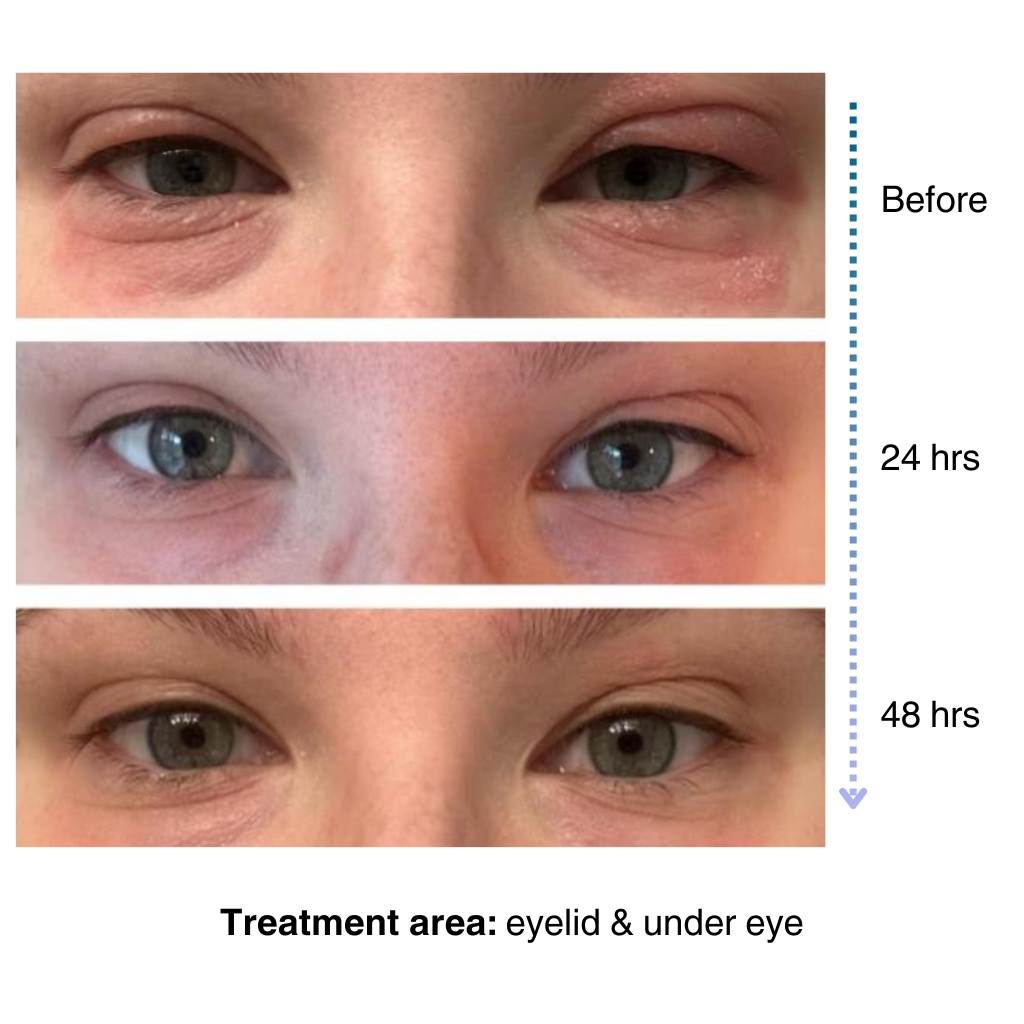
It’s easy to apply and isn’t chalky at all. I’ve been applying it multiple times a day… I’ve tried multiple new products to try and treat my eye eczema, and this is definitely the best I’ve tried so far.
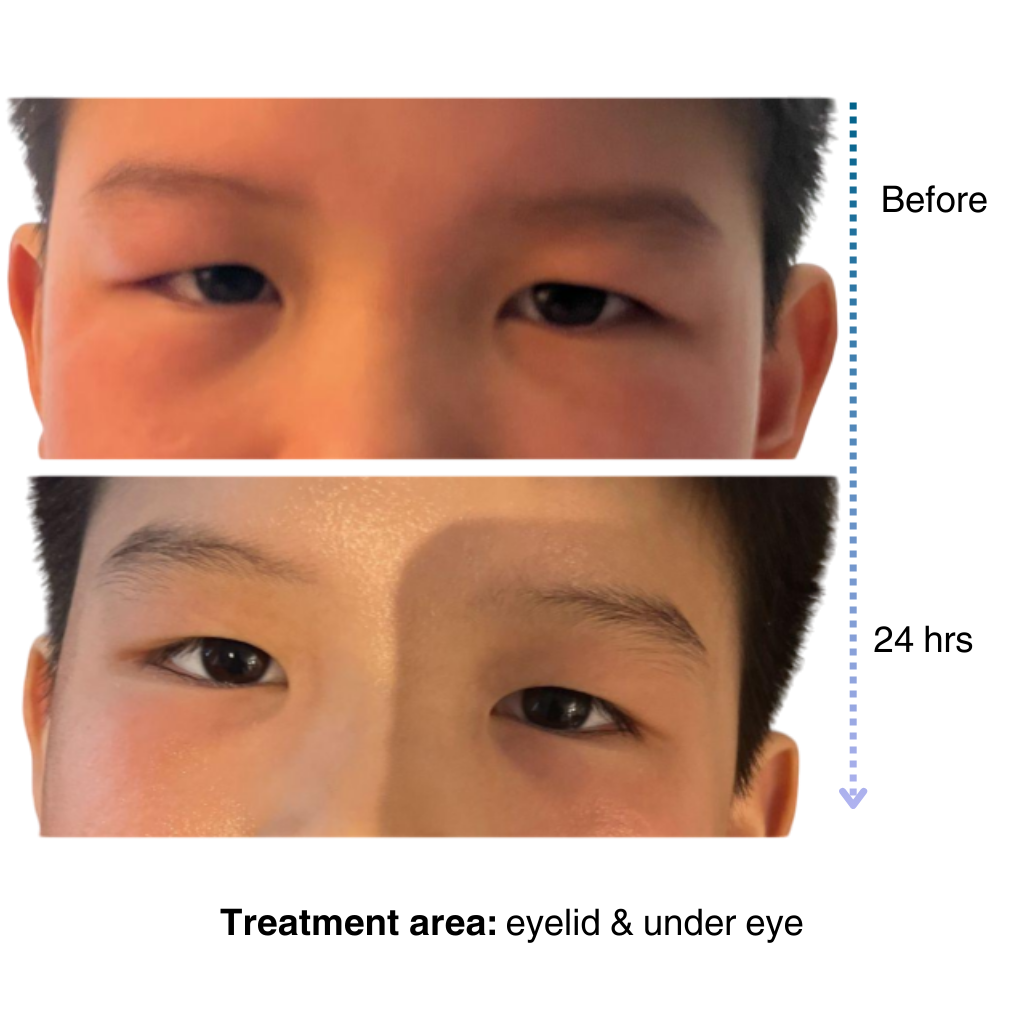
My 7-year old son has been dealing with eczema on his face for a long time, and it’s been so tough to find something that really works…..I’m amazed by the results! Within one day, the redness and rough patches on his face significantly improved…. he doesn’t mind using it at all because it doesn’t sting or feel greasy. – Lily

Like many of you, our eczema journey is personal. That’s why we’re committed to creating a space for the eczema community to share experiences, be empowered through evidence-based solutions, and learn practical tips for daily life.
– Sajjad, Founder & CEO of NellaDerm
